


Osteochondritis dissecans (OCD) is a developmental orthopedic condition in which the bone beneath the cartilage does not form properly, creating a weak area. A small flap of cartilage can separate from this weakened area with normal activity which leads to inflammation and pain. OCD of the caudal humeral head is by far the most common location, but it can develop on the caudal glenoid of the scapula.
Young, rapidly growing large and giant breed dogs are most commonly affected. Clinical signs develop once a cartilage flap forms which typically includes a consistent forelimb lameness that worsens with activity and improves with rest.
OCD is a heritable disease so the breeder should be made aware if your dog develops this disease.

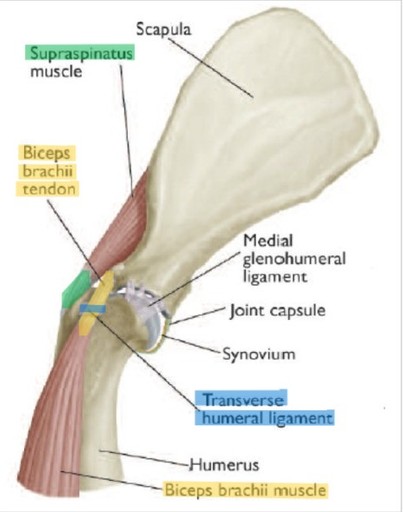
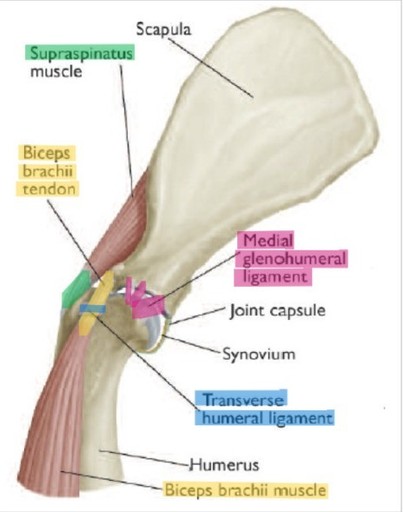
Normal Canine Shoulder

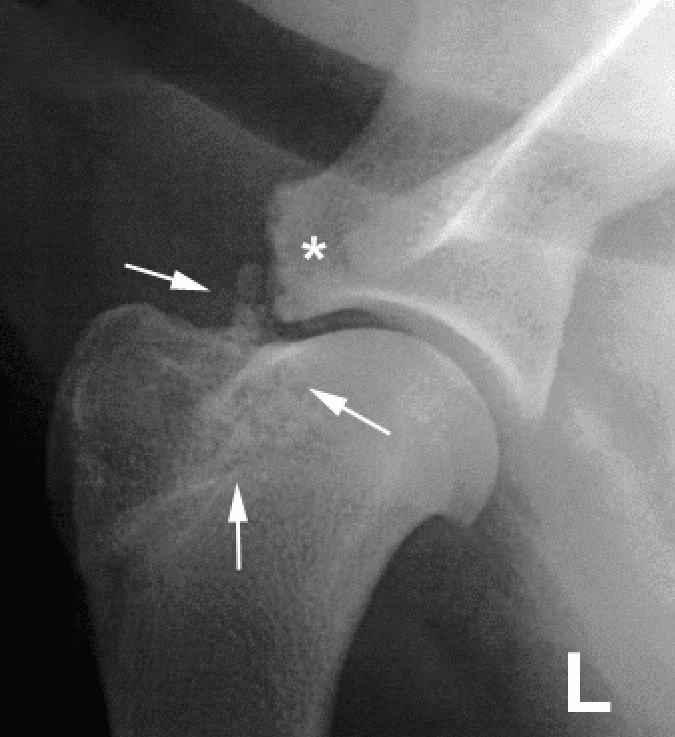
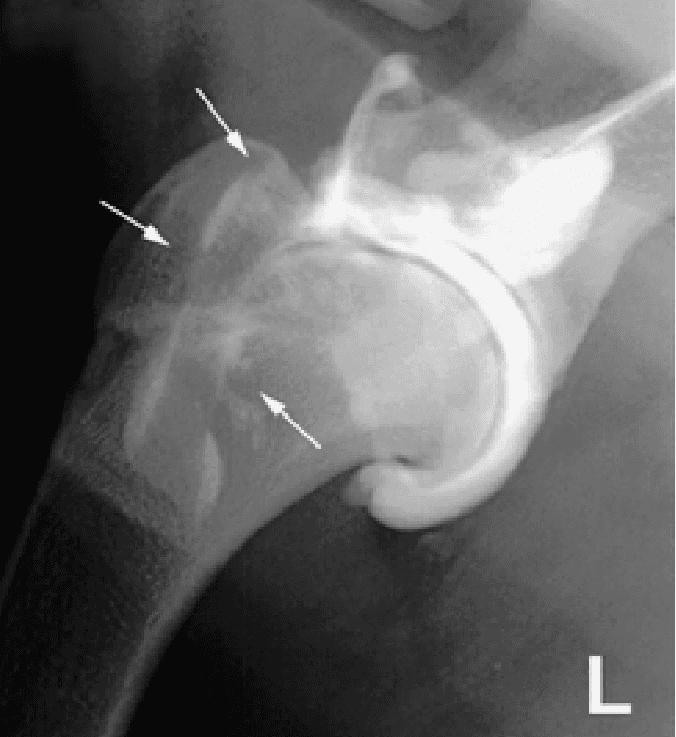
OCD of the Humeral Head
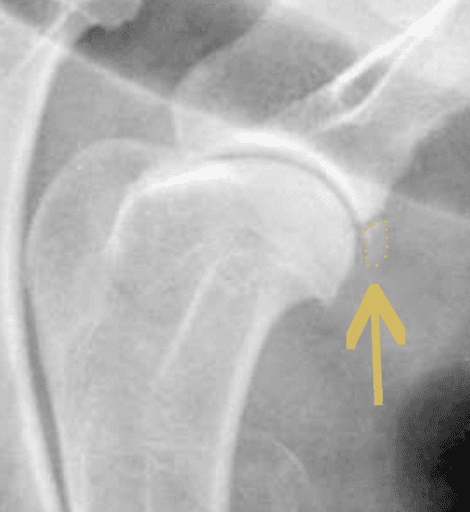
OCD of Caudal Glenoid
Diagnosis:
The disease is suspected when pain is elicited on flexion of the shoulder with physical examination. An x-ray of the shoulder is usually enough to confirm the diagnosis. In some cases, a CT scan may be recommended to identify small lesions not clearly visible on x-rays.
Both shoulders should be evaluated because OCD will commonly affect both limbs.
Treatment options include surgical fragment removal or non-surgical (conservative) management. Surgery is generally recommended, as it reliably relieves pain and minimizes the risk of long-term joint problems.
Non-surgical (Conservative) Management
Non-surgical, conservative management for OCD is unique compared to most orthopedic conditions. The partially attached cartilage flap will sometimes release during normal, high-impact activity.
If the fragment settles in an area where it does not interfere with joint function, lameness may resolve. However, the flap can migrate between joint surfaces or under the biceps tendon, leading to recurrent pain. Non-surgical management is unpredictable in how long it takes for signs to resolve and problems can arise in the future, so surgical removal is generally recommended.
Surgical Management:
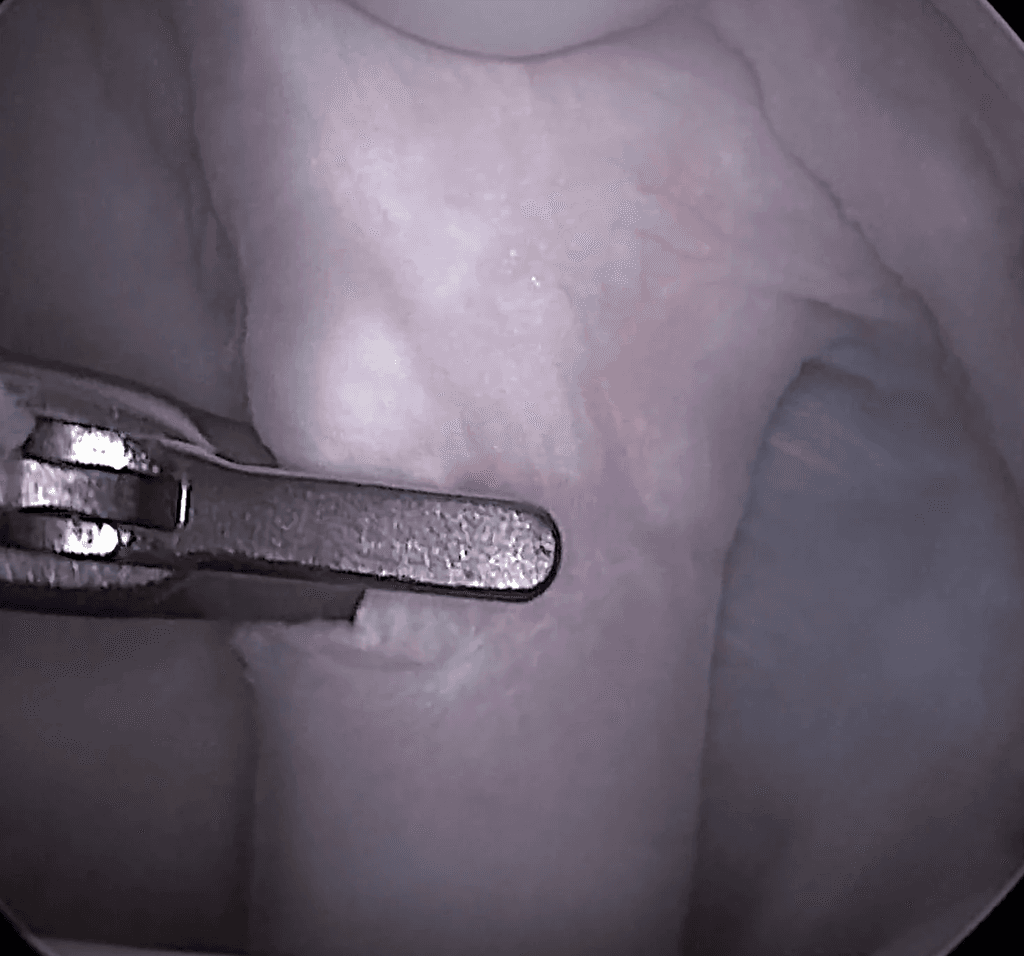
Fragment Removal
Fragment removal can be performed minimally invasively with arthroscopy or through a small open approach. Removing the fragment is the most consistent way to resolve lameness and reduce the risk of long-term joint issues. In rare cases with very large defects, a cartilage resurfacing technique may be considered, though this is seldom necessary.
Following surgery, exercise is restricted for approximately 6 weeks to allow healing of the cartilage defect.

Prognosis and Outcome:
Non-surgical management carries a highly variable and unpredictable outcome. Improvement can take weeks to months and may not be permanent, with the risk of recurrence due to fragment movement or ongoing arthritis.
Surgical removal of the OCD flap has an excellent success rate, with approximately 95% of dogs returning to normal activity once healed. Mild arthritis may still develop over time, but it is typically well-tolerated and does not significantly affect quality of life.
Biceps Tendinopathy involves irritation or damage to the biceps tendon which affects the tendon’s ability to glide through the biceps groove. This can occur either from sources within the joint, like wear and tear damage to the biceps tendon itself or irritation from a migrating OCD lesion. Alternatively, impingement of the tendon can occur outside of the joint from sources like a mineralized supraspinatus tendon.
Signs can be mild with intermittent lameness after heavier days of activity up to a significant lameness that is persistent despite activity restrictions.
Diagnosis:
Diagnosis is generally made on examination with pain elicited on palpation of the biceps tendon when the elbow is extended and shoulder flexed, which stretches out the tendon.
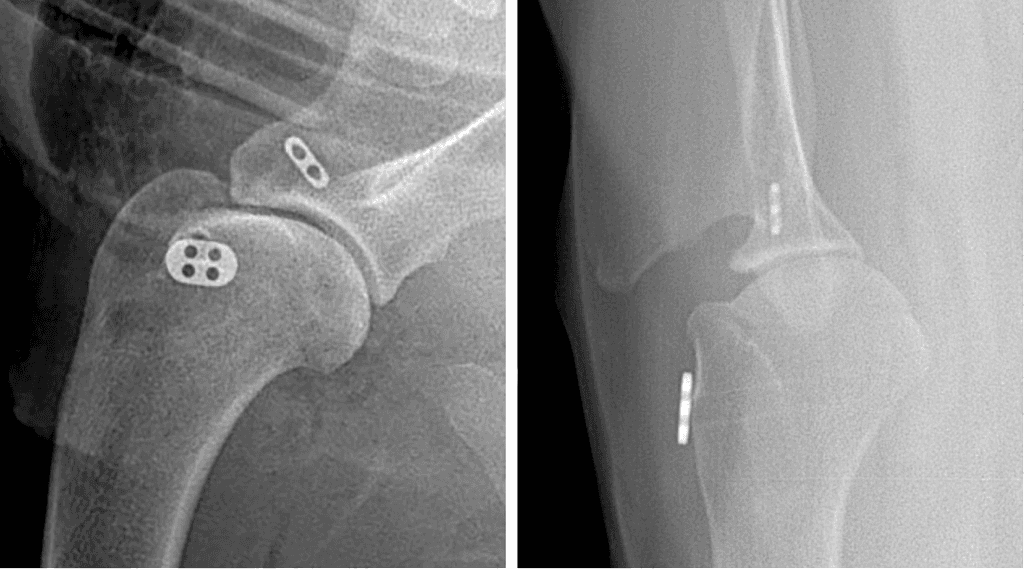
X-rays can show mineralization of the tendon or where it attaches to the scapula. Advanced imaging with ultrasound, CT scan, or MRI can be performed but are not generally necessary.
Treatment almost always begins with non-surgical, conservative management involving activity modifications, weight management, pain medications, and rehabilitation. If signs are severe, progress, or fail to respond to non-surgical management, then a tendon release can be performed to eliminate pain.
Non-surgical (Conservative) Management:
In mild to moderate cases, the goal is to stimulate tendon healing with rehabilitation but allow sufficient time for the healing before returning to normal activity.
Weight Management
Activity modifications: Limit any running, jumping or playing. Prioritize low-impact activities like leashed walks and controlled swimming.
Rehabilitation: Highly recommended to perform shockwave and laser therapy to stimulate tendon healing
Pain medications as needed
Supplements: Glucosamine/Chondroitin, omega-3 fatty acids, etc.
Most dogs with mild to moderate signs will see improvement of their signs, if not complete resolution. However, ongoing at-home rehabilitation exercises are important to maintain strength because there is always a chance of reinjury and recurrence of signs.
Surgical Management:
Biceps Tendon Release
In more severely affected patients or in those that fail to see improvement with rehabilitation, surgical intervention is warranted. The biceps tendon can be released, or cut, at the location where the impingement and pain is occurring. The cut tendon will then reattach itself further down the humerus. Function does not change because other structures around the shoulder take over the role of the biceps tendon. Rehabilitation is still important to help build strength and stability of the forelimbs to limit chances of other soft tissue injuries in the future.
Your surgeon will discuss the most appropriate option for your pet based on severity of signs, lifestyle, and overall health.
Mild to moderate cases undergoing consistent rehabilitation generally see a good response to treatment. Resolution of signs can take time but most return to normal activity. However, like any soft tissue injury, a reinjury can occur so long-term conservative management with STRICT weight management, limiting high impact activities, and continuing rehabilitation exercises at home will help to limit this risk.
Most dogs will see improvement in their comfort following biceps tendon release within the first few weeks. Often these dogs will have some degree of arthritis in either the elbow or shoulder or other soft tissue issues so signs may not completely resolve but are usually dramatically better. Ongoing conservative management with weight management, activity modifications, and rehabilitation exercises will be important to optimize functional outcome long-term.
Medial Shoulder Instability
Medial shoulder instability involves damage to the supporting structures of the medial collateral ligament and subscapularis muscle/tendon. The resulting damage leads to instability of the shoulder which causes pain and decreased function. The damage either occurs with chronic, repetitive use (agility, hunting, or other consistent high impact activities), trauma, or overload from an abnormally shaped joint (shoulder dysplasia in small dogs). In severe cases, the shoulder can become completely luxated.
Signs depend on the severity of the damage and range from a mild, intermittent lameness with activity or a consistent toe touching to non-weight bearing lameness.
Diagnosis:
Diagnosis involves demonstrating excessive mobility (abduction) of the shoulder on examination or with x-rays. X-rays often have no changes unless shoulder dysplasia is present.
Definitive diagnosis can be challenging in more mild cases because of a lack of instability and may be presumed based on history, consistent discomfort with shoulder abduction and lack of other issues.

Treatment:
Treatment almost always begins with non-surgical (conservative) management involving activity modifications, weight management, pain medications, and rehabilitation. If signs are severe, progress, or fail to respond to non-surgical management, then surgical intervention may be necessary
Non-surgical (Conservative) Management:
In mild to moderate cases, the goal is to stimulate tendon and ligament healing with rehabilitation but allow sufficient time for the healing before returning to normal activity. Activity modifications involve limiting high impact activities and prioritizing low impact activities for at least the next few months. Rehabilitation is highly recommended to help adjust the way the dog moves, strengthen the forelimbs, and stimulate healing with shockwave and laser therapies. A supportive shoulder brace can help to limit abduction and facilitate the healing process.

Surgical Management:
Medial Collateral Reconstruction
In severe cases, or those failing to see improvement with non-surgical management, reconstructive surgery may be recommended. The ligament is either reconstructed with suture material, or the biceps tendon is transposed to 'replace' the collateral ligament. The repair is protected for 2-3 weeks in a non-weight bearing bandage then careful rehabilitation begins. A supportive shoulder brace is used consistently for at least an additional 2-3 months alongside rehabilitation. Activity is restricted for a minimum of 8-12 weeks to allow complete healing of the reconstruction but some recoveries can take 4-6 months.
Humeral Head Ostectomy
Reserved for small to medium sized dogs where the joint cannot be reconstructed adequately. The procedure removes the humeral head and part of the scapular joint surface. A “false joint” forms as the surrounding muscles and soft tissues take over joint function.
Postoperative rehabilitation is essential—especially in larger dogs—to achieve a good functional outcome and should begin 10-14 days postoperatively. The goal is pain relief rather than perfect joint function, though some dogs have a good functional outcome

Shoulder Arthrodesis
In severe cases where the joint cannot be reconstructed or reconstruction fails, then a shoulder arthrodesis (fusion) may become necessary. The joint surfaces of the shoulder are removed then the shoulder completely fused used bone plates and screws. The stabilization will be protected by at least 6-8 weeks in a splinted bandage. X-rays are evaluated at 8 and 12 weeks to assess fusion then activity is slowly returned to normal.
Prognosis and Outcome:
Mild to moderate cases undergoing consistent rehabilitation generally see a good response to treatment. Resolution of signs can take time but most return to normal activity. However, like any soft tissue injury, a reinjury can occur so long-term conservative management with STRICT weight management, limiting high impact activities and continuing rehabilitation exercises at home will help to limit this risk.
Reconstruction techniques are challenging and inconsistent results are seen, so we try to avoid this procedure when possible. Approximately 60% of dogs will see a return to normal activity with good functional outcome, 25% have an acceptable outcome and the remainder will continue to have disability. It is a very long recovery and rehabilitation is extremely important to ensure appropriate healing. The repair will be protected with bandages and supportive braces which need to be maintained vigilantly. Exercise restrictions are extremely important during the healing process to limit risk of failure.
Humeral head ostectomy is an uncommon procedure generally used in small dogs with shoulder dysplasia. It is very effective at improving comfort and eliminating pain but asymmetry to the dog’s gait should be expected. No bandages or supports are necessary in the postoperative period. Consistent rehabilitation is very important and helps achieve the best functional outcomes.
Shoulder arthrodesis (fusion) effectively improves comfort and, in many cases, will improve function in the severely affected. The repair will be protected with splinted bandage for the first 8 weeks and exercise restricted for 12-16 weeks to allow adequate fusion. Once the splint is removed, rehabilitation can begin to train them how to move appropriately with the shoulder fusion. The biggest risks are implant infection (<5%) or implant failure (<1%) which can be limited with strict adherence to postoperative recommendations.
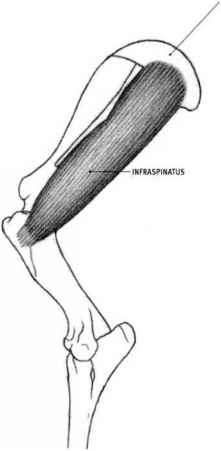
Infraspinatus Tendon Contracture
Infraspinatus contracture is an uncommon disease that almost exclusively affects hunting and working breed dogs. It begins with an acute injury to the infraspinatus musculotendinous structure that is observed as a sudden forelimb lameness in the field. The lameness will resolve on its own but then a gait abnormality develops weeks to months later. The dog will hold the paw out to the side and is unable to internally rotate at the shoulder. The initial injury to the infraspinatus heals inappropriately, resulting is a thick, tight fibrous band.
Diagnosis:
Diagnosis is made by visual assessment of gait and stance.
The limb is held externally rotated. Examination will reveal a loss of the infraspinatus muscle mass and an inability of the shoulder to internally rotate.
X-rays are usually normal.

Surgical management with tenectomy is the treatment of choice. Infraspinatus tenectomy involves removing a small section of the infraspinatus tendon which releases the muscle and allows normal shoulder motion to resume. Exercise is restricted for 10-14 days then gradually returned to normal over another 2 weeks.
Outcomes are very good with dogs almost uniformly returning to normal activity.


